Industrially processed carbohydrates
In a nutshell
Eating too much industrially processed carbohydrates creates body fat
Constantly raised insulin and insulin resistance result in “chronic disease”
Replacing industrially processed carbohydrates with real food can stop the harmful cascade

When I started writing this blog, I described my heart disease as a symptom of malnourishment caused by eating too much industrially processed food. My view on that point has not changed, although I now understand more clearly the difference between the real food we evolved to eat and process traditionally and the industrially processed products I used to consume. I also now simply categorise industrially processed products as follows:
Seed oils
Sugars and starches
Refined grains
I previously described the risks associated with seed oils here and here. In my opinion, they are the most harmful of all the industrially processed products.
In this post I’m going to describe what I understand to be the way that readily absorbed processed carbohydrates also lead to malnutrition.
The irony of dietary carbohydrates
Dietary carbohydrate is not essential for the human body [1]. This makes sense from an evolutionary point of view since our ancestors became adapted to a diet that was 70% animal protein and fat and in which carbohydrates played only a fallback role when their primary source of food was scarce.
This dietary need for carbohydrate should not be confused with biological need. For example, the human brain does require carbohydrate in the form of glucose. However, the human liver (and to a lesser extent the kidney) can provide this glucose by converting non-carbohydrate substances present in the body.
The roles of the three macronutrients in human health are summarized in Table 1.

Table 1: Biological role of dietary macronutrients (modified from reference 1)
Bioavailable dietary carbohydrates
To keep things simple, I’m going to limit this discussion to the way in which glucose is absorbed or created by the human body. We get glucose directly from real food such as certain vegetables, ripe fruit, and honey. We also get glucose indirectly from natural foods after we digest things like dairy and starches (e.g., root vegetables).
Problems arise when we expose ourselves continually to industrially processed ingredients (Tables 2 and 3) which result in very high levels of blood glucose.
For the time-being, I’m ignoring the effects of non-absorbable carbohydrates such as fibre that bypass human absorption and are fermented by our gut microbiota.

Table 2: A selection of healthy and unhealthy dietary carbohydrates from Human metabolism

Table 3: Processed carbohydrates arranged as categorised food types [2]
Is Glucose the problem?
Think of it this way. If one of us falls off a tall building, the fall isn’t the problem, it’s the sudden stop at the bottom. Consumption of industrially processed ingredients delivers a constantly high payload of glucose. It’s what our body does as a consequence that is the problem.
When our blood glucose is increased, our body responds by producing the hormone insulin to keep blood glucose within safe limits and to move it to where it can be used or stored for later use.
Unfortunately, the human metabolism is not adapted to cope with constant and heavy exposure to glucose. Our insulin response can’t cope and becomes the problem.
The central role of insulin and insulin resistance
Insulin
Let’s begin by reminding ourselves what insulin is. I previously wrote:
“Insulin is the main hormone involved in human metabolism, and may determine whether we are healthy or not.
Insulin has two main roles. Firstly, it keeps our blood glucose level within a safe range, ensuring that we have enough for our energy needs and that it does not become dangerously high. Insulin’s second role is analogous to a very dynamic and interactive traffic light essentially ensuring that the macronutrients available are used for energy…”
I still stand by that description. However, in describing insulin resistance I was wrong to characterize it as wholly a bad thing.
Insulin resistance
There are two types of insulin resistance (IR), acute and chronic. Acute IR (IRA) is healthy whereas chronic IR (IRC) creates harm if left unchecked.
IRA is an important state to which we are adapted. IRA was evolutionarily important during times of food shortage (e.g., winter) to ensure that the parts of us which need lots of glucose (e.g., retina, red blood cells) received more than organs which could more readily use fats (e.g., brain). IRA is also associated with pregnancy and puberty. In all cases, IRA is not only necessary, it is reversible [1].
I now understand that I was previously referring to IRC when I stated:
“Constantly high levels of insulin means that our cells are always being signaled to take up more glucose for energy. It also means a constant signal to our liver to create fat for long-term storage. Our body fat cells eventually stop responding to the insulin signal at which point fat may be stored in our livers. This process of ever-higher insulin being ignored by our cells becomes the vicious cycle that is insulin resistance.
Insulin resistance represents a disintegration of the glucose-insulin signaling mechanism at the centre of healthy metabolic flexibility and it is associated with a range of so-called chronic diseases…”
Persistent blood insulin
When suffering from IRC we develop persistently high blood insulin. This state goes by the daunting term hyperinsulinemia.
The combination of IRC and persistently high blood insulin are believed to underpin many so-called “chronic diseases” (Figure 1).
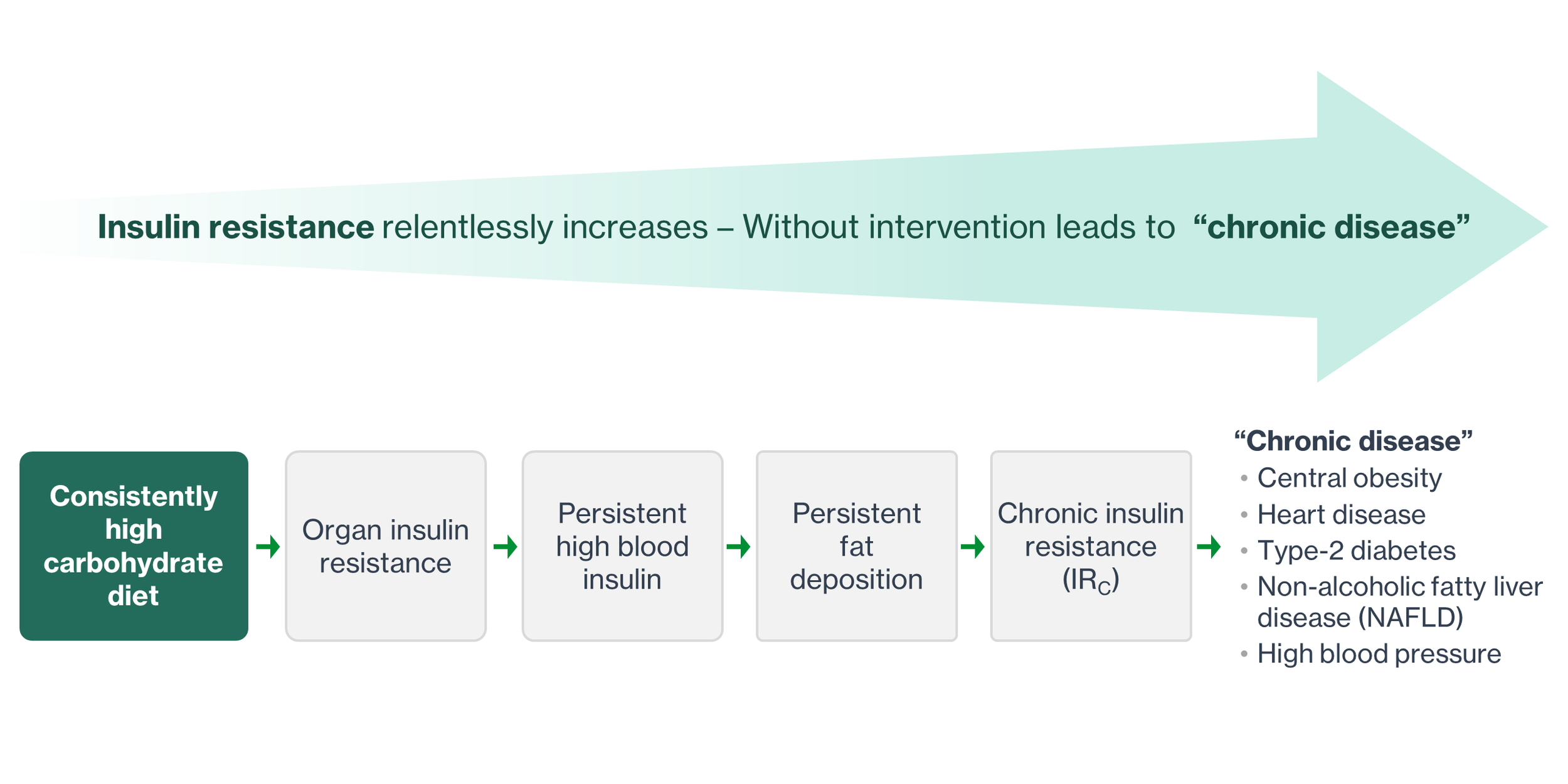
Figure 1: IRC and raised insulin from eating high carbohydrate food leads to “chronic disease”
Persistent blood insulin and IRC lead to range of “chronic diseases”
Figure 1.12 in Chapter 1 of the book Ketogenic [1] lays out in considerable detail the ways in which high carbohydrate diets can create malnutrition and lead to a range of “chronic diseases”. I was eventually able to understand it but failed utterly to recall the important steps along the way. I decided, therefore, to simplify the authors’ excellent diagram and summarise more simply. My summaries are presented in Figures 2 – 5. Necessarily I’ve eliminated much subject-matter terminology and many details. Anyone interested in the subject will do well to read the book themselves.
I’ve reduced the overall process of carbohydrate-induced malnutrition into three stages as follows:
Consistently high processed dietary carbohydrates cause persistent high blood insulin and body fat (Figure 2)
Persistent fat creation leads to ectopic obesity, chronic inflammation, and IRC (Figure 3)
IRC leads to obesity, Type-2 diabetes, heart disease, high BP, and NAFLD (Figure 4 and 5)
In considering the ways in which eating too much processed carbohydrate can lead to “chronic disease”, two themes consistently pop-up. Firstly, the problem is associated with ever-increasing blood insulin, IRC, and chronic inflammation. Secondly, the are many places in the harmful cascade where action may be taken to halt the damage.
Consistently high dietary carbohydrates cause persistent high blood insulin and body fat
When we consume more carbohydrates than we need for energy, the liver converts blood glucose to fat for storage. Usually, we store fat under our skin. However, our normal fat reserves become insulin resistant and less sensitive to the instruction from blood insulin and we start to store fat unhealthily in the liver, muscles, and pancreas. This unusual storage is called ectopic fat.
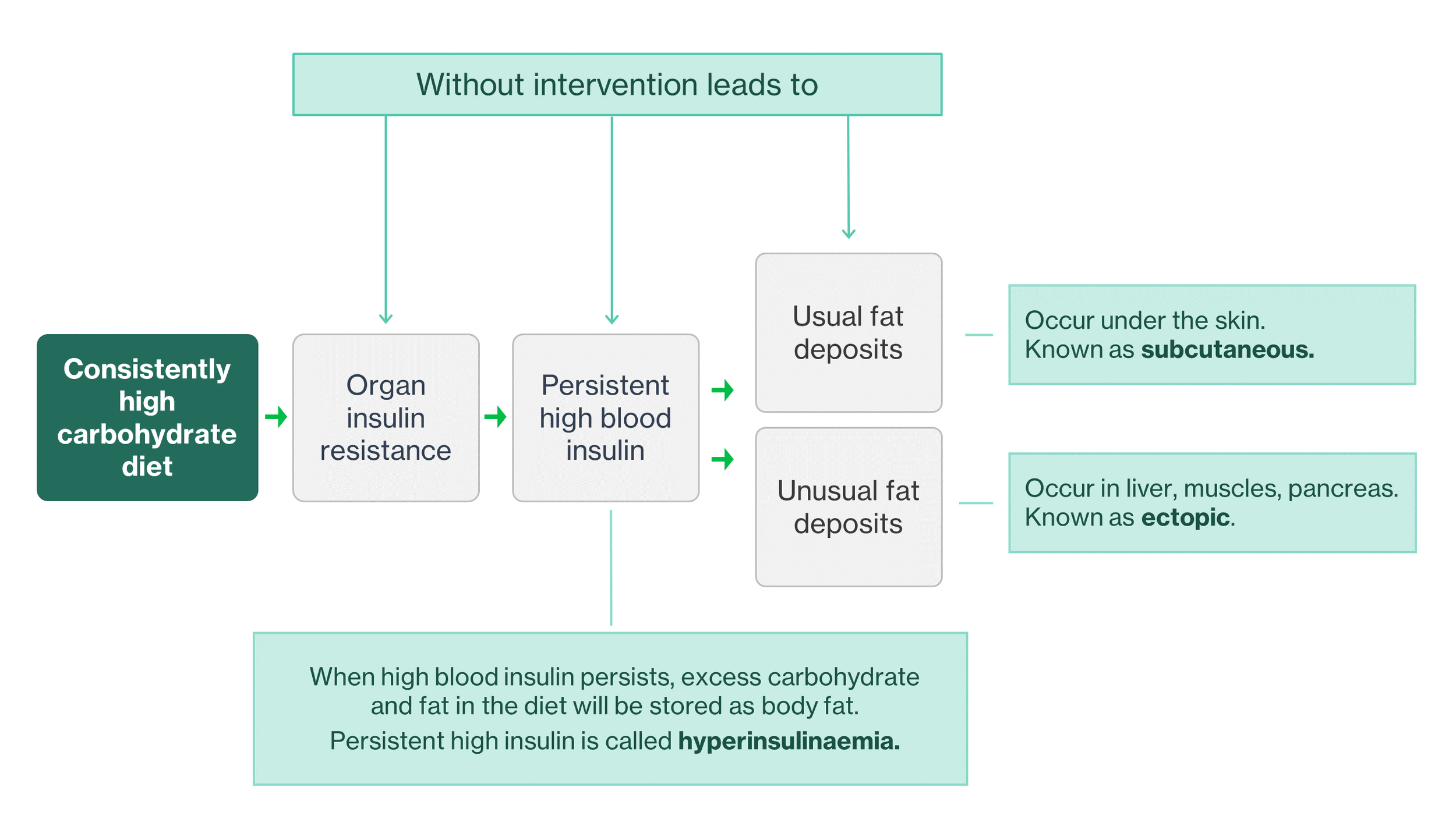
Figure 2: Eating too much processed carbohydrate food results in unhealthy body fat
Persistent fat creation leads to ectopic obesity, chronic inflammation, and IRC
Under the continual onslaught of a high processed carbohydrate diet, insulin resistant fat cells start to enlarge abnormally. Those abnormally large fat cells then start to behave in ways that are harmful. They stop producing a healthy hormone (adiponectin), and instead release proteins that cause inflammation. Both lead to ever more IR and ectopic obesity, and a vicious cycle ensues. The reduction in adiponectin results in fat being released into the blood also.

Figure 3: Insulin resistant fat create an unhealthy metabolism which leads to IRC
IRC leads to obesity, Type-2 diabetes, heart disease, high BP, and NAFLD
Ectopic fat in the liver is called non-alcoholic fatty liver disease (NAFLD) which is itself considered to be a “chronic disease”.
With IRC the liver signals to fat cells in a way that causes them to make IR even worse, compounding the problem. The liver also tries to get rid of its ectopic fat but unfortunately releases damaged cholesterol in the process, leading to potential heart disease. IRC also causes the liver to over-produce glucose and this cascades ultimately to the development of Type-2 diabetes (Figure 4).
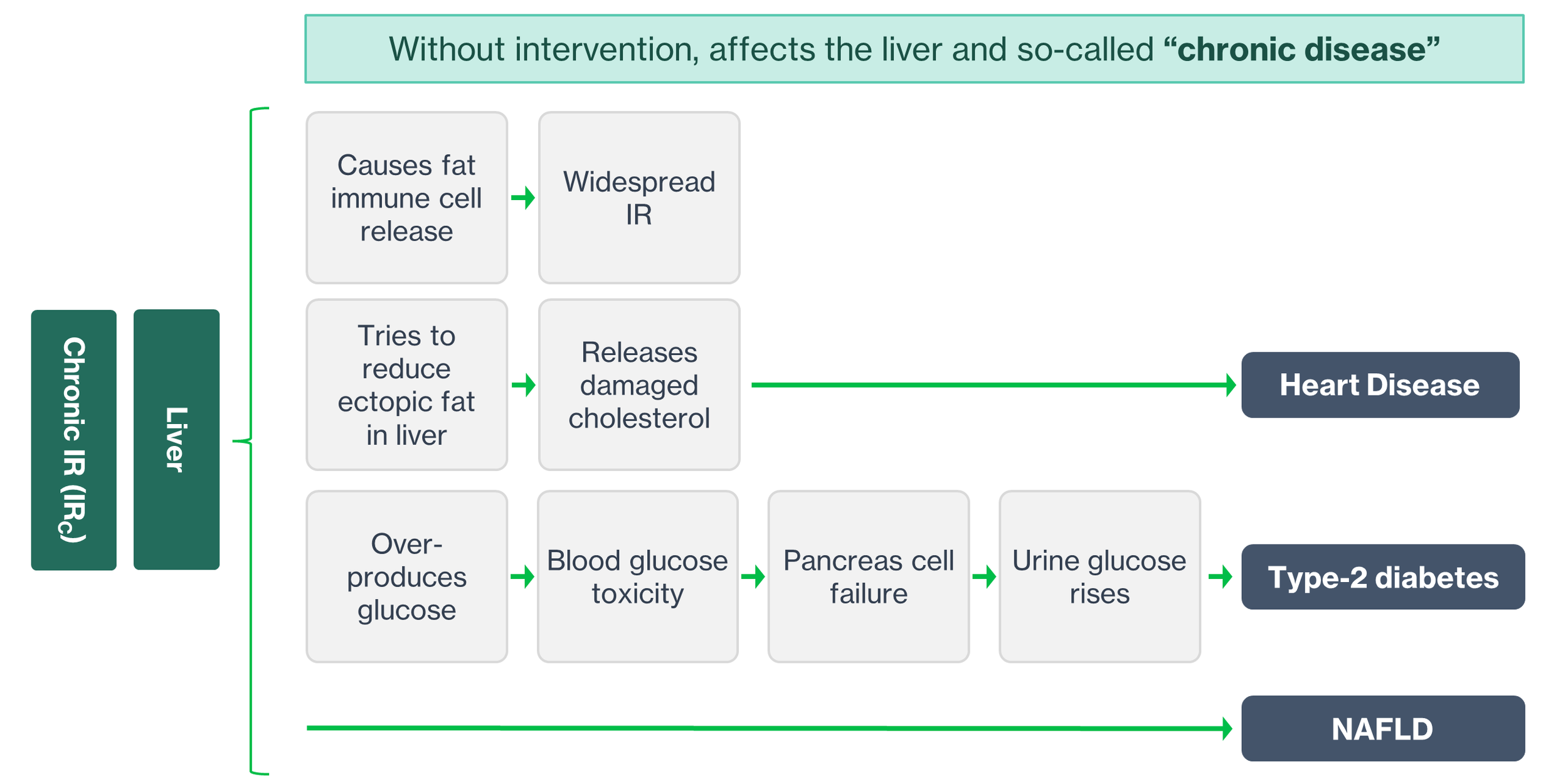
Figure 4: IRC creates NAFLD and can also lead to heart disease and Type-2 diabetes
Whilst much of the damage caused by IRC emanates from the liver, it is not the only organ ivolved in “chronic disease” when we eat too much processed carbohydrates. For example, enlarged fat cells are essentially implicated in central obesity, the pancreas in Type-2 Diabetes because of its influence on the liver, and the adrenal glands in high blood pressure. A brain influenced by IRC may also be harmed, albeit not in a way that is recognized by the medical community as “chronic disease”.
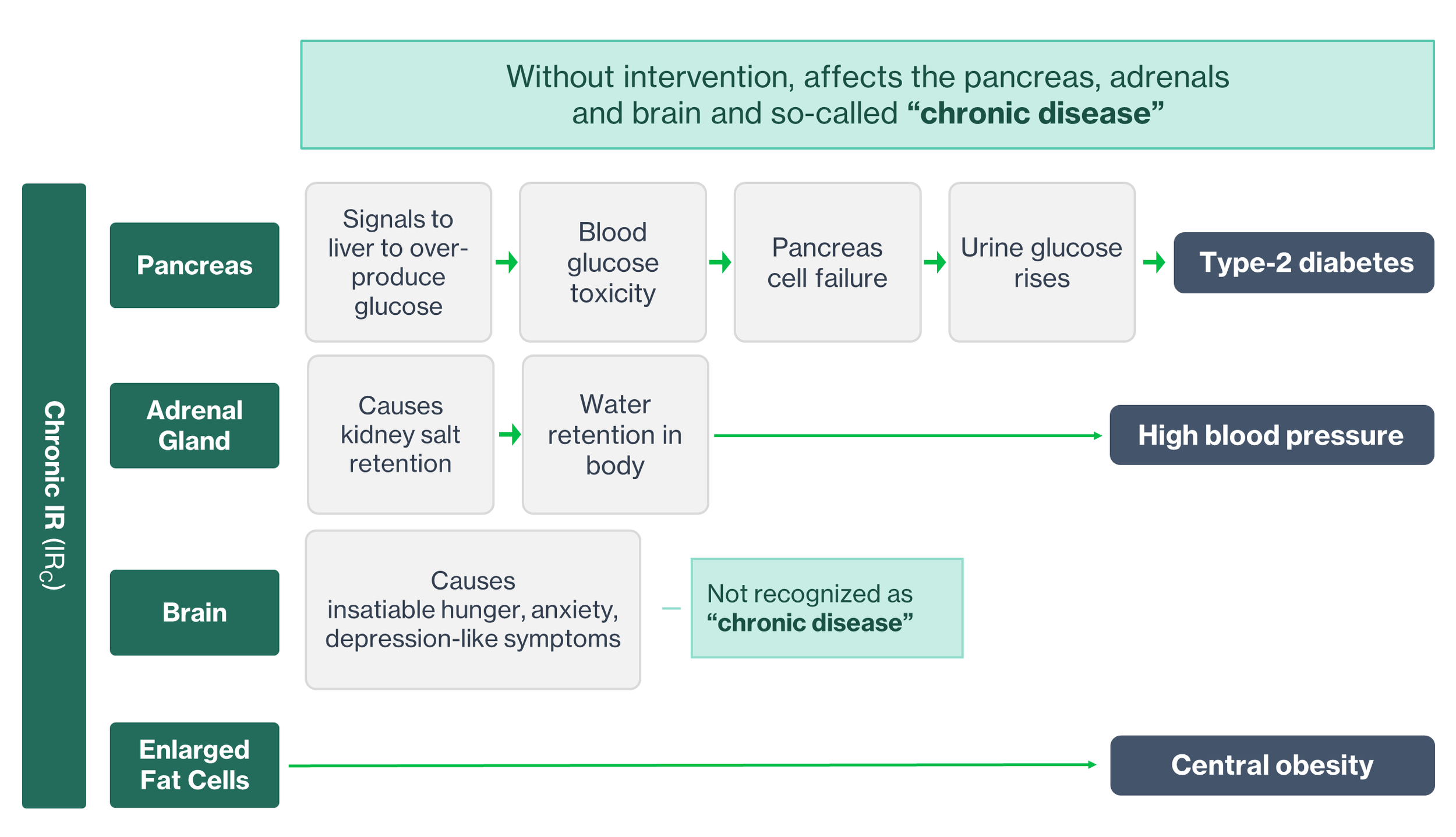
Figure 5: IRC creates obesity and can also lead to high BP
How to intervene
Figures 2 and 3 show several places within the harmful cascade of ever-increasing IRC and chronic inflammation where the damage may be at least slowed, stopped, and perhaps reversed. This might be achieved by eliminating highly bioavailable dietary carbohydrates or fasting.
Eliminating highly bioavailable dietary carbohydrates
An obviously helpful step might be to cut out readily absorbed, industrially processed carbohydrates (Table 2 and 3) and replace with real food. This is what I chose to do years ago.
I’m impressed by what has been described in the management of Type-2 diabetes and mental health.
David Unwin is a leader in the treatment of Type-2 diabetes and has given many sufferers hope in its treatment. From a recent publication:
“The authors examined a group of 186 type-2 diabetes patients at their medical practice over a period that averaged just under three years. Within the first year of the study, the team of doctors found that 77% of patients following a low carbohydrate dietary regime were able to reverse their disease. By the end of the study, 51% of their patients had maintained reversal of type-2 diabetes by changing what they ate.”
Additionally, Gary Taubes in his excellent new book [3] describes the results of the Virta Health clinical trial as follows:
“It had demonstrated that the degeneration of the diabetic condition could be reversed, even that the disease itself could be put into a drug-free remission with continuous remote care and a diet that restricted carbohydrates and replaced those calories mostly with fat”
In the field of mental health, Christopher Palmer in his excellent book Brain Energy provides a number of case studies.
“My personal favourite is the story of Mildred, a seventy-year-old obese schizophrenic patient. Her doctor advised the ketogenic diet for weight loss and after just two weeks she began to lose weight and noticed an improvement in her psychotic symptoms. Now, thirteen years later, she has learned how to take care of herself, is 150 pounds lighter, symptom-free, and not taking her old medications.”
Fasting
Fasting can be defined as voluntarily not eating for a defined period [4]. Technically, breakfast is the meal we use to break our fast between last eating the previous day and our first meal of the new day. I tend to observe a daily 16-hour fast in what can also be described as time-restricted eating.
I’ll address fasting in a future blog but for the time-being, look at reference 4 if you’re interested.
Summary
If we consume too many processed carbohydrate ingredients, over time we can cause harm to ourselves. As I think about this, I’m not terribly surprised. We used to call processed food “junk” for a reason.
I grew up thinking about what I ate every day and the possibility of developing a “chronic disease” as two separate things. Starting seven years ago I was forced to consider that I’d been wrong all my life and that the things I ate were the root-cause of my heart disease. My diet of industrially processed carbohydrates delivered to me a payload of consistently high glucose. My human metabolism responded appropriately and tried to control my blood glucose. The ensuing storm of ever-increasing high insulin and chronic insulin resistance did me in.
Modern, processed carbohydrates wouldn’t be a problem if I possessed a body that was adapted to cope with them. Unfortunately I don’t, in fact no human alive today has a body that is adapted to consume such a diet without repurcussions.
I’m actively eliminating those ingredients listed in Tables 2 and 3 as much as possible to reduce the effects of my “chronic disease”. We’re all different and what works for me may not be for you and vice versa. I do think the evidence against eating too much carbohydrate junk food is compelling, however.
References
Noakes, T.D. et al (2023) Nutritional Fundamentals. In Noakes, T.D., et al, editors. Ketogenic: The Science of Therapeutic Carbohydrate Restriction in Human Health. London, Academic Press, PP. 3-70
Kong, W. et al (2024) Higher ultra processed foods intake is associated with low muscle mass in young to middle-aged adults: a cross-sectional NHANES study Front. Nutr., Volume 11 https://doi.org/10.3389/fnut.2024.1280665
Taubes, G. (2024) Rethinking Diabetes: What Science Reveals about Diet, Insulin and Successful Treatments. London, Granta Publications
Fung, J. et al (2023) Therapeutic fasting. In Noakes, T.D., et al, editors. Ketogenic: The Science of Therapeutic Carbohydrate Restriction in Human Health. London, Academic Press, PP. 469-484